AUCTORES
Globalize your Research

Case Report | DOI: https://doi.org/10.31579/2690-4861/144
*Corresponding Author: Chithra Ram, Neuroradiologist, Assistant Professor, Department of Radiology, University of Louisville, Kentucky, USA.
Citation: C Ram, H Moss, M Terry, M Kannan, R Sherry. (2021) Multi-Modality Imaging of Craniofacial Fibrous Dysplasia with Orbital Complications and Histopathology Correlation-A case report and short review of literature. International Journal of Clinical Case Reports and Reviews. 7(3); DOI:10.31579/2690-4861/144
Copyright: © 2021 Chithra Ram, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 08 June 2021 | Accepted: 22 June 2021 | Published: 25 June 2021
Keywords: craniofacial fibrous dysplasia; ct of craniofacial fibrous dysplasia; mri of craniofacial fibrous dysplasia; mri perfusion of fibrous dysplasia; fibrous dysplasia imaging; histopathology of fibrous dysplasia
Craniofacial fibrous dysplasia [CF-FD] with orbital complications is a known but rare entity. This is a multi-modality imaging Case Report of extensive CF-FD in a 31-year-old male with right eye pain, swelling, and redness, along with histopathology correlation. In this patient, the CT scan demonstrates the classic ground glass bony appearance in great detail and helps with the diagnosis of FD, while excluding other bony pathology. The patient’s corroborative MRI brain with and without contrast and MRI brain perfusion images are presented to further characterize this pathology along with its orbital and ocular complications. Given the significant mass-effect on the ocular structures, the patient underwent orbital surgery with removal of as much of the lesion as possible. On macroscopic pathology evaluation, the affected bone was rubbery and gritty when sectioned. Microscopically, remnant fragments of woven bone of various size and shapes were seen with lack of an osteoblast rim. The bony fragments had a characteristic curvilinear, trabecular, and/or branching pattern. Post-surgical imaging demonstrated improvement in the mass-effect on orbital structures and proptosis, along with residual bony lesion.
Fibrous dysplasia [FD] forms 7% of benign bone tumors. FD usually presents within the first two decades of life. However, our patient was over 30 years of age. It has no gender predilection. Approximately 85% of cases of fibrous dysplasia are associated with activating missense mutations in GNAS gene with stimulation of adenylyl cyclase and over-expression of cAMP. FD can be monostotic or polyostotic. Monostotic lesions are most common. A very small percent of these lesions can be large enough to cause complications. E.g. involvement of a large portion of the orbital walls with mechanical compression on the orbital structures resulting in related signs and symptoms, etc.Craniofacial involvement may occur both as monostotic or polyostotic fibrous dysplasia. Occasionally it is seen in McCune-Albright syndrome.
A 31-year-old male presented to the emergency department with right eye pain, swelling, and redness that began the prior morning. There was no history of trauma and he denied any visual disturbances. Prior medical history was significant for hypertension. Vital signs were notable for a blood pressure of 179/92. Physical exam showed a large solid lesion in the right fronto-orbital region and proptosis. Neurologic examination showed decreased sensation to light touch on the right side of the face. The rest of the body including the extremities were unremarkable. CT and MRI were obtained to evaluate the right fronto-orbital lesion.
CT head without contrast was performed in a Somatom Definition Edge Siemens scanner [Siemens Medical Systems, USA]. Standard 1mm axial CT soft tissue and bone detail algorithm images were obtained followed by reconstructed images in coronal and sagittal planes.
MRI of the brain was performed on a 3T Siemens Spectra scanner [Siemens Medical Systems, Malvern, Pennsylvania, USA] using a standard head coil. Standard 4 mm thick axial T1, axial T2, fat suppressed axial T2 FLAIR, axial DWI and ADC brain pulse sequences were acquired without contrast. After intravenous administration of 20 ml of Multihance, perfusion imaging was performed along with axial and coronal post contrast T1W sequences.
IMAGING FINDINGS
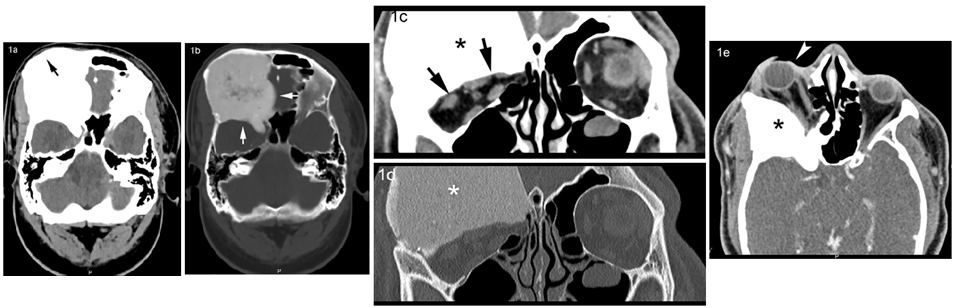
CT examination of the brain showed a large, expansile, sclerotic lesion in the right orbital roof and sphenoid bone with infiltration of the ethmoid sinuses characterized by benign appearing margins and a uniform classic “ground-glass” appearing matrix (Fig.1a,b). The bony contour of the right supraorbital region was smoothly expanded. The expansile right orbital bony lesion compromised the total volume of the right orbit and caused severe proptosis (Fig. 1c, d, e), mass-effect on the extra-ocular muscles particularly lateral rectus and probable optic nerve compression due to the narrowed optic canal.
IMAGING FIGURES: Craniofacial Fibrous dysplasia
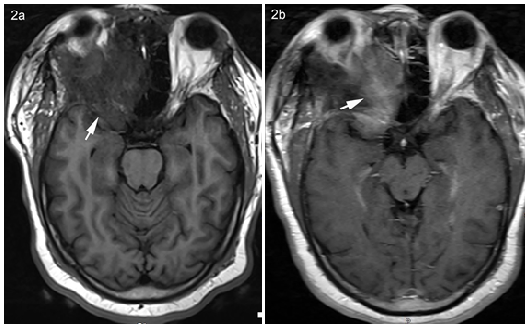
The MRI appearance was in keeping with CT diagnosis of FD. It showed heterogeneous T1 hypointensity and mild diffuse enhancement after contrast administration (Fig. 2). Additional MRI perfusion imaging (Fig. 3a) confirmed that this was not a vascular lesion and helped exclude vascular lesions such as metastasis or meningioma. DWI sequences revealed no restricted diffusion (Fig. 3b, c). Based on the imaging findings and clinical presentation the lesion was felt to be consistent with CF-FD. The patient underwent subtotal resection of the large skull lesion with decompression of the orbit, optic nerve, and superior orbital fissure using microsurgical technique and intraoperative neuronavigation. Thin layers of the lesion were unable to be resected due to their close proximity to the frontal and ethmoid sinuses. Subsequent cranioplasty with titanium mesh was used to create the orbital rim (Fig. 4). Post-operatively he developed moderate vision loss in the right eye. Follow-up postoperative imaging showed no expansion of the fibro-osseous lesion. His most recent 7 years post-op imaging shows stable and unchanged remnants of the fibrous dysplasia and proptosis. No other intervention since initial craniotomy has been necessary.


HISTOPATHOLOGY FINDINGS
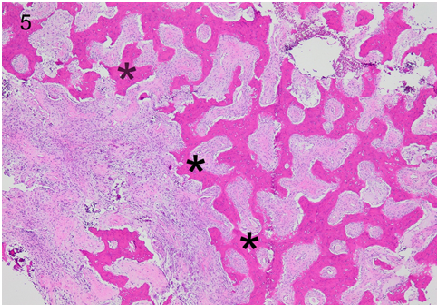
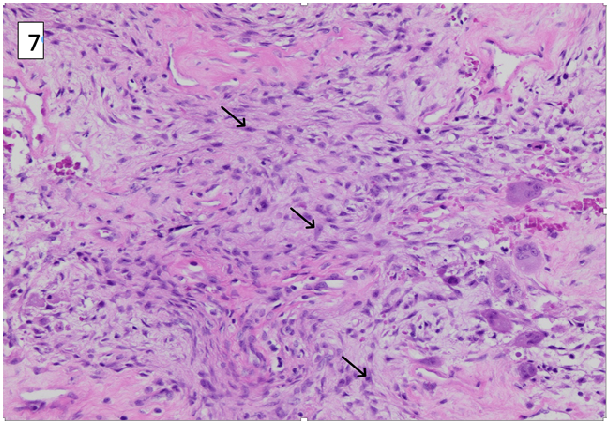
In the 4X low power hematoxylin and eosin (H&E) stained slide of the specimen [Fig.5], a combination of fibrous appearing tissue and scattered bony trabeculae were well seen. The 10X mid power H&E stained slide [Fig.6] demonstrated areas of hemorrhage associated with multinucleated osteoclast-type giant cells. Matrix resembling cementum was found in this craniofacial lesion. 20X High power H&E stained slide [Fig.7] demonstrated moderately cellular stroma with storiform [whirling] and spindle shaped cells. Fibrous dysplasia was diagnosed based on the moderately cellular spindle cells arranged in storiform (cartwheel or whirling) pattern with low mitotic count amidst the woven, discontinuous bone trabeculae.

INTRODUCTION
Fibrous dysplasia [FD] is a well-known benign bony entity. It is a developmental disorder that results from a sporadic mutation that replaces bone with fibrous tissue, resulting in structural instability [1]. FD can be monostotic [involvement of one site] or polyostotic [involvement of 2 or more sites], with monostotic lesions being most common [2,3]. Craniofacial involvement in FD can be monostotic in 10-25% of monostotic cases or polyostotic in up to 50% of polyostotic cases. FD can also exist in conjunction with endocrinopathies (e.g. McCune-Albright Syndrome) [4]. Polyostotic FD is more commonly associated with symptomatic disease and deformity [5]. It's a non-hereditary disorder with expansile lesion(s) caused by a defect in osteoblastic differentiation and maturation. It contains a mixture of fibrous tissue and woven bone, giving rise to the characteristic ground glass appearance. Sarcomatous dedifferentiation can be rarely seen in polyostotic FD with prior radiation therapy.
McCune-Albright Syndrome has a clinical triad of polyostotic FD, hyperfunctioning endocrinopathies and café au lait spots. It has a female preponderance [7]. Mazabraud Syndrome is polyostotic FD with intramuscular myxoma. It has increased risk of malignant transformation. Cherubism is familial FD involving bilateral jaw [8].
CLINICAL PRESENTATION
FD is often asymptomatic and diagnosed incidentally as a well-circumscribed lesion, especially with monostotic disease. Clinical presentation often depends on location and number of lesions. Ribs, femurs, and craniofacial bones are most commonly affected [3,6]. Craniofacial FD presents with asymmetric facial enlargement due to the affected bone, proptosis, atypical facial pain or numbness, headache and cranial neuropathy (diplopia, hearing loss, blindness) [9]. Progression from monostotic disease to polyostotic has not been documented [1]. Craniofacial bones are most commonly implicated in monostotic FD, while the femur is commonly affected in polyostotic FD. Polyostotic disease occurs in a younger age with limp, leg pain, or pathologic fractures. The lesions are commonly unilateral and are located in the same extremity when the appendicular skeleton is affected [8]. Fractures typically occur at the proximal femur with possible “shepherd’s crook” deformity. If the spine is affected, then scoliosis can occur [3,6]. Patients with café-au-lait spots and precocious puberty with FD should be considered for a diagnosis of McCune–Albright syndrome [10]. Association with aneurysmal bone cysts has also been described [11].
IMAGING FINDINGS
Commonly discovered as an incidental finding, lesions of fibrous dysplasia are characterized into three types [12]. Pagetoid lesions are most common, followed by sclerotic and then cystic lesions [7]. In craniofacial FD, more than 1 bone involvement is often seen. Maxilla, orbit, and frontal bones are commonly involved, while ethmoids and sphenoids are rarely involved. CT is most sensitive and specific. CT and MR help define local extent, while bone scintigraphy scan identifies additional lesions [10].
Radiographs: FD is a smooth, well circumscribed, homogeneous ground glass lesion with well-defined borders. Endosteal scalloping and cortical thinning is noted due to the expansive nature of the lesion. It may be sclerotic or lucent (cystic). Sclerotic lesions are homogenously dense. Cystic lesions can show a “rind” sign, where a thick layer of sclerotic reactive bone surrounds a lucent lesion [3,7,14]. This sign is commonly seen in proximal femur.
CT: Radiolucent ground-glass matrix in an expansile bony lesion involving the medulla, is diagnostic especially in pagetoid lesions. Smooth cortical contour is typically maintained. Endosteal scalloping may also be present [13].
MRI: Decreased T2W signal is noted throughout the lesion if it's pagetoid or solid type and only in rim if it's of the cystic type. Increased pathological activity can result in fewer bony trabeculae and hence result in increased T2W signal [3,7]. Decreased T1W signal is usually seen. Enhancement is variable. It can be peripheral, diffuse or non-enhancing.
Bone scan: It's nonspecific with variable radionuclide uptake in perfusion and delayed phases. It's sensitive but not specific in identifying skeletal lesions in polyostotic FD.
PET: FD shows variable uptake on FDG [Fluoro-deoxy glucose] PET. Correlation with CT helps differentiate it from metastasis.
HISTOPATHOLOGY
The histopathologic features of CF-FD consists primarily of normal bone that is replaced and distorted by bland fibrous tissue [15]. Grossly, the affected bone is rubbery and gritty when sectioned [15]. Microscopically, remnant fragments of woven bone of various size and shapes are seen. These bony fragments characteristically lack an osteoblast rim, and may seamlessly interface with adjacent cancellous bone or cortex [15,16]. As a result, there may be no clear demarcation between lesion and adjacent normal bone on imaging [17]. The bony fragments are curvilinear, trabecular, and/or branching, which gives a characteristic “Chinese letter” or “alphabet soup” appearance [15]. This manifests as diffusely distributed opacities on imaging. The bone fragments are typically trabecular or woven, although lamellar bone is occasionally present if the lesion has been present for many years [15-17]. The fibrous tissue is relatively cellular and contains spindled or stellate fibroblasts with associated collagen. Mitotic figures are scarce or absent [15]. Cases with abundant cartilage, named fibrocartilaginous dysplasia, have been described [15]. Synonyms that are no longer recommended for use include osteitis fibrosa, fibrous osteoma, and unilateral von Recklinghausen disease. Approximately 85% of cases of fibrous dysplasia are associated with activating missense mutations in GNAS gene with stimulation of adenyl cyclase and over-expression of cAMP [15,18].
PROGNOSIS AND TREATMENT
Prognosis is good, many cases spontaneously resolve with aging as the lesions become inactive after puberty, and the condition is considered benign. Asymptomatic cases can be managed with patient education and clinical observation [19]. The maintenance of bone density is important during management, especially for prevention of fractures [1]. Malignant transformation can rarely occur and is more common in polyostotic rather than monostotic FD [7]. No treatment methods are currently available to slow or alter the disease course. Bisphosphonates can control bone pain [19]. Polyostotic patients should be carefully monitored to optimize function and ambulation as they can result in pathological fractures, which may affect mobility. Surgery with grafting is an option to correct deformities or otherwise symptomatic lesions and large monostotic lesions can be resected [3,19]. Aggressive resection is reserved for visual loss and severe deformity of the cranium.
FD is a benign congenital condition that results in replacement of normal bone architecture with fibro-osseous tissue. The condition can be monostotic or polyostotic and can be in association with endocrine abnormalities in the context of McCune-Albright Syndrome and Mazabraud Syndrome. Disruption of bone structure predisposes these patients to deformity and fracture, but the overall prognosis is good. Radiologists should be aware of the potential for some of these lesions to rarely undergo malignant transformation in polyostotic FD cases. The characteristic ground-glass appearance on CT is pathognomonic. In this patient the MRI perfusion images were useful in confirming the avascular nature of the lesion and in helping to exclude potential vascular lesions such as Paget’s disease, metastatic disease and invasive meningioma. Most patients can be managed conservatively, with surgical options reserved for those with extensive deformity, fracture, or malignant transformation. In the patient reported here, surgical intervention was necessitated by the severe mass-effect on the ocular structures from the expansile bony lesion with resultant proptosis, eye pain, redness and potential for optic nerve compression.
ABBREVIATIONS
FD - Fibrous dysplasia, CF-FD – Craniofacial Fibrous dysplasia, CT - Computerized Tomography, MRI - Magnetic Resonance Imaging. PET – Positron Emission Tomography.
CONFLICT OF INTEREST: None.
FUNDING: None.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.
